|
"Review of Recent Literature " Othmer, Kaiser and Othmer
EEG Biofeedback
Training for Attention Deficit Disorder:
A Review of Recent Controlled Studies and Clinical Findings
Siegfried Othmer, Ph.D., David Kaiser, Ph.D., and Susan F. Othmer,
B.A.
June, 1995
Introduction and Summary
One of the fastest-growing applications of biofeedback at the present
time is the use of EEG biofeedback for the remediation of attention
deficits ( Attention Deficit Hyperactivity Disorder, ADHD), related
behavioral disorders, and specific learning disabilities. This is
happening largely on the basis of the continuing work of Joel and
Judith Lubar, of Michael Tansey, and of a growing core of clinicians.
The knowledge base is expanding primarily through increasing clinical
use of the technique, rather than through controlled research. The
lack of contemporary, large, suitably controlled studies has, however,
inhibited acceptance within the larger psychological, psychiatric,
and educational communities.
Efficacy of the EEG training for ADHD has been ascribed variously
to remediation of the underlying condition of physiological underarousal
manifesting in hyperactivity (Lubar, 1976); to addressing the motor
component of hyperactivity by changing the set-point of the motor
system with training at sensorimotor cortex [the same mechanism
proposed for motor seizures (Sterman, 1980)], or by training the
supplementary motor area responsible for the initiation of movement
(Tansey, 1990); and to remediation of disregulation of arousal manifesting
variously in inattention or behavioral disinhibition (Othmer, 1994).
The validity of one of these mechanisms does not rule out validity
for another. Indeed, they may each be responsible for addressing
some aspect of ADHD symptomatology.
In the following, some recent studies will be briefly reviewed,
and a statistical analysis of data coming out of current clinical
practice will be presented. The clinical findings leave the matter
of efficacy for ADHD beyond any reasonable doubt. The results are
so robust that they cannot be attributed to a placebo effect, or
other nonspecific effect of the training. However, the controlled
studies to date have been much more ambiguous in their outcomes.
Some possible explanations of these differences are presented.
Return to Introduction * Recent Findings * Clinical Findings *
Results * Discussion
Recent Findings of Controlled Studies
Several studies have surfaced recently which meet criteria for controlled
studies, and which therefore are beginning to fill the vacuum. Michael
Linden has performed two studies which have both documented statistically
significant shifts in IQ scores, along with favorable behavioral
changes, using training protocols derived from Lubar. In his first
study, which involved a small group of 9 experimental subjects and
9 controls, Linden found an increase in I.Q. scores of 10 points,
with a statistical significance of p < .05, using the Kaufman
Brief Intelligence Test, or K-BIT (Kaufman, 1990) (Linden, in press).
He also found an improvement in parental assessment of inattention,
likewise with p < .05. Hyperactivity improved to where it was
below the abnormal rating; however, the change was not statistically
significant. Assessments used the SNAP rating scale (Swanson, 1981)
and the IOWA-Conners rating scale (Atkins, 1987). Training protocol
was reinforcement of 16-20 Hz, with concurrent inhibition of excess
4-7 Hz activity. Training extended over 40 sessions. The findings
were replicated in a second study, which is currently in preparation
for publication.
Henry A. Cartozzo reported on his thesis work at the annual meeting
of the Association for Applied Psychophysiology and Biofeedback
(Cartozzo, 1995), which involved a small controlled study of EEG
Biofeedback for ADHD using a protocol derived from Lubar (augmentation
of 12-15 Hz activity with inhibition of 4-7 Hz and 22-30 Hz, with
placement at Cz). Training extended over thirty sessions. Using
8 subjects and 7 controls, Cartozzo found significant improvements
in the subtests of the WISC-R intelligence test which are most closely
identified with ADHD, namely Arithmetic, Digit Span, and Coding.
Together with Information, which was not tracked, the above WISC-R
subtests constitute the famous "ACID" test of ADHD.
The WISC-R results obtained in the Cartozzo study are shown in Table
1, with comparative data from previous studies (Tansey, 1990; Othmer,
1991). The WISC-R changes were found to be significant at the level
of p < .01, whereas the control group showed no significant changes.
The results also fall in line with the previous studies. How may
we interpret these results? The three subtests are associated with
a factor called "Freedom from Distractibility". And they
are the ones most sensitive to difficulties in sequential processing.
Hence, improvement in these scores can be interpreted in terms of
improvement in the continuity of mental processing, in working memory,
and in the ability to sustain attentional focus. These improvements
would, in turn, be observed as a diminution of distractibility.
A minor criticism may be advanced: The latest data suffer from the
fact that the two groups were not matched in starting subtest scores.
The control group had lower mean scores than the experimental group.
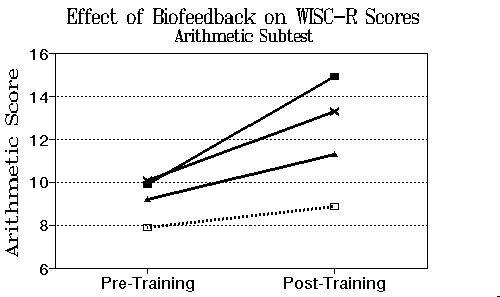
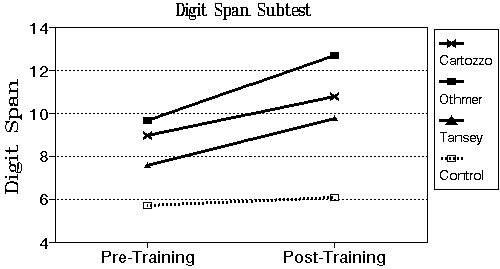
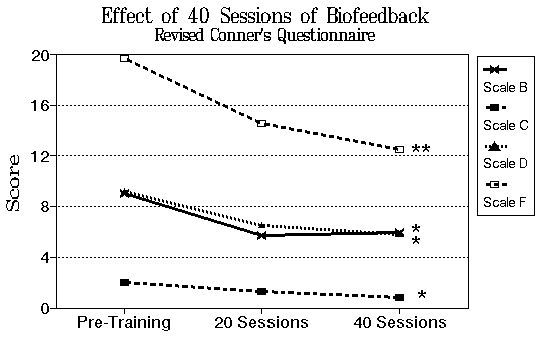
Figure 1. Improvements in WISC-R subtest score for three independent
studies (Cartozzo, 1995; Othmer, 1991; Tansey, 1990) employing similar
EEG training protocols.
The Cartozzo study also found improvements in scores on a computerized
continuous performance test, the T.O.V.A. (Test of Variables of
Attention) (Greenberg). The improvement in attention score was significant
at the level of p < .01. The control group showed no significant
movement on that test. The study also found behavioral improvements,
but scores remained in the abnormal range even after the training.
Furthermore, the control group improved on most behavioral measures
even more than the treatment group. All changes were significant.
However, they failed to confirm the expected interaction with treatment
condition. On the other hand, amplitudes in the 4-7 Hz regime did
decline with the training, whereas they increased in the control
group. Amplitudes within the training band of 12-15 Hz did not change
significantly over the course of training. The biofeedback cohort
was given feedback via a PAC-Man like object which encoded the feedback
signal in terms of its brightness and velocity through a maze. The
control group was given the conventional PAC-Man game for the same
number of sessions.
One hesitates to propose video games as a remedy for the disregulated
behaviors of ADHD on the basis of the above behavioral improvements!
There is a better interpretation of these findings. The Cartozzo
study restricted itself to a single protocol in the study. This
was unfortunate, since it is already known that different children
may need different protocols (Lubar, 1991). The result is that some
children improve while others do not, or may even deteriorate in
behavior. This manifested itself in an increase (near-doubling)
in the standard deviation of scores in the experimental group (whereas
the standard deviation remained unchanged in the controls). The
behavioral changes were reduced in statistical significance because
of this increase in dispersion of the data.
Finally, Aubrey Fine and Larry Goldman of California Polytechnic
Institute in Pomona (Cal Poly) reported preliminary results on their
controlled study of ADHD at the 1994 annual meeting of the American
Psychological Association in a poster presentation. This study involved
two experimental groups, one getting EEG biofeedback, and a second
obtaining cognitive training with a computerized tool (Captain's
Log). A third group was a wait-list control. Because this was an
initial study of a survey nature, the intake criteria were quite
inclusive. Children were admitted who had been diagnosed not only
with ADHD but also with seizure disorder, Tourette Syndrome, and
depression. Most were already under medical management for these
conditions. Some 80% of the group were medicated, 15% of them with
more than one medication. Some of the remaining 20% of children
were on summer drug holiday.
Because of the multiple objectives of the research study, assessment
tools included the Wide Range Assessment of Memory and Learning,
Stroop Color and Word Test, Kagan Familiar Figures Test, and the
Grooved Pegboard Test. For ADHD assessment, the Conner's CPT and
the Gordon Diagnostic System were employed, in addition to several
parent questionnaires (Child Behavior Checklist, Home Situations
Questionnaire, Child Attention Profile, Revised Conner's Questionnaire,
and Social Skills Assessment).
Few of the academic skills tests revealed statistically significant
improvement in either of the experimental conditions (12/51). Of
course, the population had not been selected for deficiencies on
those measures in the first instance, so it is difficult to judge
the import of this finding. With respect to the ADHD assessments,
the Conner's CPT showed improvement in omissions (inattention),
commission errors (impulsivity), and response time. However, so
did the control group! No statistically significant interaction
with treatment condition was identified. The Gordon Diagnostic System
did not yield significant change.
Parental Assessments, however, indicated some significant favorable
changes. The Conner's Questionnaire yielded improvement on the impulsive-hyperactivity
scale at the p < .01 level for the EEG training contingent. This
finding is taken to be highly significant for several reasons. First,
the behavioral improvement was identified in a population that was
largely already medicated for ADHD, as stated above. Secondly, it
was identified after only 20 training sessions, which is generally
acknowledged to be insufficient to achieve a full resolution of
ADHD with EEG training (Lubar, personal communication). Thirdly,
it was identified by parents strictly on the basis of the home environment,
since the first 20 training sessions were conducted over the summer
months. For many of the children, the home environment is not as
challenging as the school environment, so it would be harder to
observe a change. And finally, a significant number of children
were able to reduce their medications over the course of the EEG
training. A maintenance of behavioral scores in the face of reduced
medication dose should also be judged an improvement, but would
not show up in the above statistics.
Part of the experimental group in the Cal Poly study was selected
for an additional 20 sessions of training. The remainder of the
group was composed of those who had essentially met the objectives
of the training, and those who had not made significant progress
in the first 20 sessions to merit continued training. The latter
two groups were each a quarter of the total, so that about half
(12) was selected for more training. In fact, only about 7 actually
undertook the additional 20 sessions and subsequent retest. The
results of testing after 40 sessions showed continued progress,
as illustrated in Table 2, with four measures reaching significance
at p < .05, and two reaching significance at p < .01 (hyperactive
index of Conner's, and the depression scale of the child behavior
checklist).
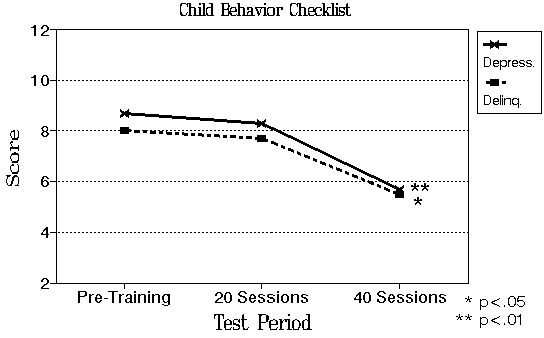
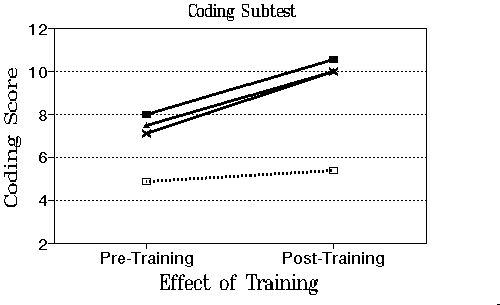
Figure 2. Effect of 20 and 40 Sessions of EEG Biofeedback on Conner's
Questionnaire Scale B (Learning Problems); Scale C (Psychosomatic);
Scale D (Impulsive Hyperactivity); and Scale F (Hyperactivity);
and on the Child Behavior Checklist depression and delinquency scales.
The last of the three groups may be regarded as "non-responders"
in the usual sense. The case can be made that the experimental data
should be evaluated also on the basis of a division between "responders"
and "non-responders", as is typical in drug studies [Introduction
* Recent Findings * Clinical Findings * Results * Discussion
Findings from Clinical Operations
The next useful step which can be taken is to review the quantitative
data derived from our actual clinical setting. In the following,
T.O.V.A. data are reported which were obtained at our home office
and affiliated offices for children with ADHD or ADHD-type symptoms.
The analysis was performed by David Kaiser, who had access to the
data from nine independent offices employing identical protocol
selection criteria for this population. The protocols consist of
training to reinforce instantaneous increase in EEG amplitude in
either the 12-15 Hz or the 15-18 Hz band, at either C3, Cz, or C4,
as needed depending on the symptomatology. The augmentation training
is accompanied by inhibition of excessive amplitudes in the 4-7
Hz and 22-30 Hz regimes.
Return to Introduction * Recent Findings * Clinical Findings *
Results * Discussion
Experimental Results
Mean pre- and post-training TOVA scores are presented in Table 3
for the initial re-evaluation after 20 training sessions. A univariate
Analysis of Variance (ANOVA) was used to evaluate the effect of
EEG biofeedback training on four components of the T.O.V.A. The
four test components were Inattention (Percent Omission), Impulsivity
(Percent Commission), Response Time, and Response Variability. Because
some clinicians truncated test scores at 40 points (i.e., four standard
deviations below normal), all individuals who scored 40 points or
below were assigned the score of 40 points. A total of 239 subjects
were included in this analysis.
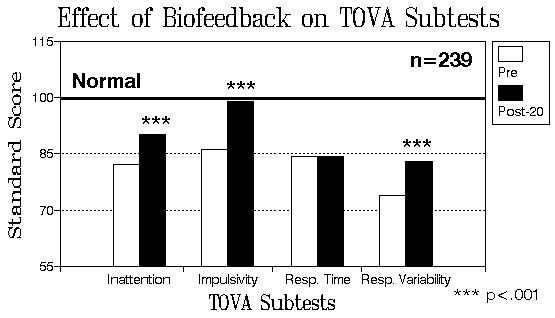
Figure 3. Mean standard scores for T.O.V.A. subtests before and
after 20 EEG biofeedback sessions for 239 children and adults.
A significant effect of EEG biofeedback training as well as an
interaction with TOVA components were observed in this data set
(p < .001). After 20 EEG biofeedback sessions, subjects improved
significantly in inattention scores (p < .0001); in impulsivity
scores, (p < .0001); and in variability of response time (p <
.0001). The mean improvement in impulsivity score is nearly one
standard deviation (15 points in standard score). Response time
does not show systematic improvement. This is partly understandable
in that subjects increase in mean response time as they reduce in
impulsivity. This dependency is documented in a regression coefficient
of -.26 between impulsivity and response time scores.
The availability of a large subject pool also allows us to evaluate
the effect of additional training sessions. Of the 239 subjects,
56 continued training and were retested after 40 or more EEG biofeedback
sessions. Understandably, these were individuals who had made only
modest progress in 20 sessions. The results are shown in Table 4.
As before, a significant effect of EEG biofeedback training (p <
.001) as well as an interaction with TOVA components (p < .01)
were observed. Compared to the pre-training scores, after 40 EEG
biofeedback sessions subjects improved significantly in inattention
(p < .05); impulsivity (p < .001); and response variability
(p < .001). When TOVA scores were compared between 20 sessions
of training and 40 sessions of training, marginal improvement was
seen in response time (p < .10); and significant improvement
was observed in response variability, (p < .001).
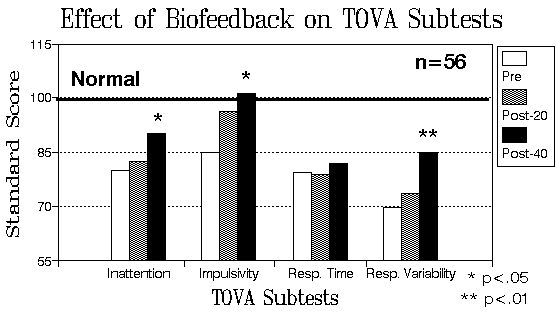
Figure 4. Comparison of T.O.V.A. subtest scores after 20 and 40
training sessions for 56 subjects who continued training out of
the 239 subjects of Figure 3.
The treatment of data on the basis of averages obscures much detail.
In particular, it weights equally those who are in significant deficit
with respect to a parameter, and those who may be normal. In Table
5, results for all 239 subjects are presented depending upon initial
pre-treatment scores. All data with starting values above the normal
score of 100 have been excluded from the table. It may aid interpretation
of these results to note that in its application to titration of
medication, T.O.V.A. score changes of a half standard deviation
(7.5 units in standard score) are taken to be significant (Greenberg).
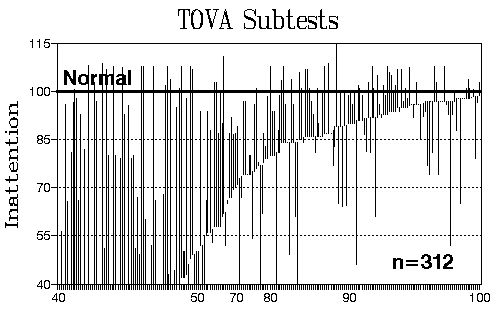
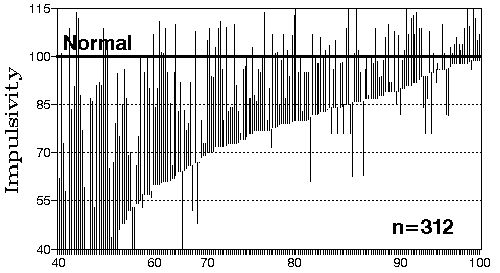
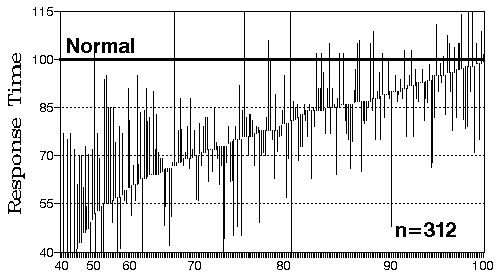
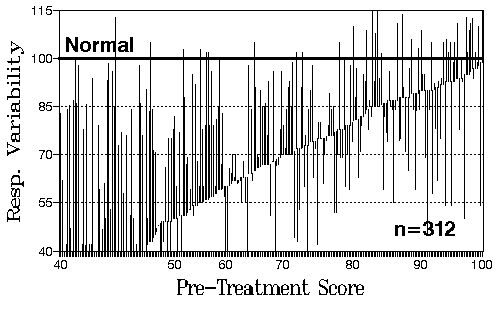
Figure 5. Results are presented for 312 subjects for changes in
TOVA subtest scores. Each line segment represents a single subject's
change from pre-training to post-training scores. The data are sorted
by pre-training score. Improvement is indicated when the line segment
rises above the pre-training value. Only individuals with pre-training
deficits in a subtest are included in each figure.
In Figure 5, there is a systematic tendency toward improvement
in all four subtests, with the most significant improvements occurring
where the pre-test scores are in most severe deficit.
Return to Introduction * Recent Findings * Clinical Findings *
Results * Discussion
Discussion
Taken together, the data from all of the studies support the model
that EEG biofeedback training is effective in changing neurophysiological
function which contributes to the symptomatology of ADHD. Improvements
in IQ scores are systematically found in all of the studies which
have looked for them, and such improvements are very difficult to
ascribe to placebo factors. Behavioral improvements were noted in
all of the studies.
The data derived from a number of clinical settings using common
protocol selection criteria also appear to be quite robust in demonstrating
changes in physiological function consequent to EEG biofeedback
training. Since these data are not matched by controls, it remains
to dispose of any placebo interpretation. First of all, the fraction
of subjects favorably impacted by the training considerably exceeds
that expected from typical placebo effects. The large study by Ullman
and Sleator, for example, found an 18% placebo response in a medication
study (Ullman and Sleator, 1986). More typically, placebo response
falls in the range of 30% of the subject population.
Secondly, much placebo response is traceable to investigator bias.
That is not present in this instance, since the testing is completely
computer-controlled and computer-scored. Thirdly, the placebo effect
can be traced to expectations on the part of the participants: Teacher
questionnaires such as those used in the Ullman and Sleator study
may be subject to such bias. Again, that cannot be the case in the
present instance. Fourth, the placebo effect is expected to be in
the direction of a favorable outcome. The data, by contrast, show
that of the few who do not show favorable change, a large fraction
actually worsen their scores to a degree not expected by normal
drift in the measurement over time. This argues for the presence
of an active agent with the potential for inducing both positive
and negative change. This is inconsistent with a placebo interpretation.
The adverse changes observed in our subjects deserve some further
comment. The essential clinical choice required for each subject
is whether to address primarily the inattention or the impulsivity.
Each of these requires its own class of protocols. If both components
are present, a compromise may be required in terms of our clinical
objectives. Hence, improvement in impulsivity may entail a worsening
of the inattention score, and an improvement in inattention may
entail an exacerbation of impulsivity. The balance may be redressed
in a subsequent series of 20 training sessions when secondary symptoms
are met with a different choice of protocols.
By virtue of this choice of protocols, each subject in a sense becomes
his own control, since an inappropriate choice of protocols may
produce adverse test results. Since a client cannot have wished
for such specific and disparate outcomes with respect to impulsivity
and inattention, of which he may himself be only dimly aware, a
placebo explanation is ruled out. A further argument against a placebo
explanation is that both Table 2 and Table 4 show continued progress
when sessions are extended from 20 to 40 sessions. A placebo effect,
by contrast, tends to fade over time.
EEG biofeedback is a physiologically based tool with essentially
no emphasis on talk therapy. The placebo effect, whatever its nature,
is psychologically mediated. It is more parsimonious to propose
that a physiologically based technique actually has a physiological
effect, than that the physiological effect is mediated by some psychological
factor such as being mesmerized by fancy instrumentation (Barkley,
1992). General psychological factors simply lack the specificity
of the tool we have at our disposal. Moreover, calling something
a placebo effect does not dispense with the issue. So what if our
effects are mediated psychologically to some degree? There are ultimately
measurable physiological consequences, the mechanisms for which
require elucidation.
When the placebo hypothesis is adduced in a test of medication efficacy,
it encompasses all "non-drug" effects. However, in its
application to a behavioral management technique, the placebo hypothesis
is an empty hypothesis. It lacks testable predictions which would
allow it to be distinguished from a postulated "real"
effect. To call something a placebo has the perverse effect of barring
further inquiry. In the absence of decision criteria and testability,
the placebo hypothesis lacks scientific utility in application to
a non-drug modality.
It remains to deal with the fact that the behavioral changes found
in the controlled studies do not appear as robust as the physiological
changes documented by the T.O.V.A. results from the clinical settings.
The Cartozzo study suffered from a small subject group, as well
as from restriction to a single protocol, as already mentioned.
The problematic finding in that study was the fact that the control
group improved its behavior significantly as well. This is perhaps
an indication of the intrinsic volatility of behavioral variables,
as well as the additional variability attributable to parental and
teacher assessment. Such variability may place fundamental limitations
on our ability to demonstrate systematic progress with training
in small populations.
The same considerations apply to the Cal Poly study. Significant
population shifts were observed in the control group with respect
to a number of test variables. This limited the significance of
any improvement in the experimental groups. This shortcoming can
be dealt with partly by greater reliance on more physiologically
based measures, such as those of the T.O.V.A., and on stable tests
such as the WISC-R. The limited significance of changes, in the
face of apparent high intrinsic variability of the measures chosen,
can only be overcome with larger "n". One way of achieving
a larger subject population is to perform a meta-analysis of the
data, such as that of Table 1, where common test instruments were
used in a number of studies. The total number of subjects in Table
1 comes to 54. It is our intention to solicit the cooperation of
the other researchers to perform such an analysis in the future.
We suggest, in summary, that the T.O.V.A. results obtained in actual
clinical settings are sufficiently cogent and robust to justify
the enthusiasm for EEG training which is building among clinicians,
and to justify the interest of academic researchers. Finally, the
above data should cause any objective researcher to desist from
asserting that clinicians may be premature in using this technique
clinically. In particular, contamination by placebo factors does
not invalidate the finding of significant improvement. A placebo
effect is inevitably marbled through everything that a clinician
does, and in fact the clinician will do everything in his power
to enhance the effect!
We expect that mental health and educational professionals will
be increasingly compelled to address the physiological basis of
behavior, as this is elucidated in research, and that EEG biofeedback
will be increasingly recognized as a useful complement to other
behavioral interventions as well as to psychopharmacology. We believe
that the discoveries now being made in the field of EEG biofeedback
portend a watershed in the field of mental health and of education
as the implications of these findings are gradually assimilated.
Return to Introduction * Recent Findings * Clinical Findings *
Results * Discussion
References
Atkins, M., and Milich, R. (1987). IOWA-Conners Teacher Rating Scale.
In M. Hersen & A. Bellack (Eds.), Dictionary of Behavioral Assessment,
Pergamon Press, New York, pp. 273-275.
Barkley, R. A. (1992). Is EEG Biofeedback Training Effective with
ADHD Children? CHADDer Box, April, p. 5-11.
Captain's Log, Sandford, J.A., 727 Twin Ridge Lane, Richmond, VA
23235 (804) 320-0105
Cartozzo, H.A., Jacobs, D., Gevirtz, R.N. (1995). EEG Biofeedback
and the Remediation of ADHD symptomatology: a controlled treatment
outcome study. Presented at the Annual Conference of the Association
for Applied Psychophysiology and Biofeedback, Cincinnati, Ohio,
March.
Fine, A. H., and Goldman, L. (1994). Innovative techniques in the
treatment of ADHD: An analysis of the impact of EEG biofeedback
training and a cognitive computer generated training. Paper presented
at the 102nd Annual Convention of the American Psychological Association,
Los Angeles, CA August 12-16.
Greenberg, L.M., Department of Psychiatry, Box 393 UMHC, 420 Delaware
Street Southeast, Minneapolis, Minnesota 55455 (612) 626-5806.
Kaufman, A. & Kaufman, N. (1990). K-BIT: Kaufman Brief Intelligence
Manual. Circle Pines, M.N. American Guidance Service.
Linden, M., Habib, T., Radojevic, V. (in press). A controlled study
of the effects of EEG biofeedback on cognition and behavior of children
with attention deficit disorders and learning disabilities. Biofeedback
and Self-Regulation
Lubar, J.O., and Lubar, J.F. (1976). EEG and behavioral changes
in a hyperactive child concurrent with training of the sensorimotor
rhythm. Biofeedback and Self-Regulation, 1, 293-306.
Lubar, J.F. (1991). Discourse on the development of EEG diagnosis
and biofeedback for attention deficit/hyperactivity disorders. Biofeedback
and Self-Regulation, 16, 201-225.
Othmer, S.F, Othmer, S., and Marks, C. S., (1991) EEG Biofeedback
Training for Attention Deficit Disorder, Specific Learning Disabilities,
and Associated Conduct Problems, EEG Spectrum, 16100 Ventura Blvd.,
Suite 10, Encino, CA 91436.
Othmer, S. F., and Othmer, S., (1994). Professional Training Syllabus,
EEG Spectrum, 16100 Ventura Blvd., Suite 10, Encino, CA, 91403.
Swanson, J., Nolan, W. & Pelham, W. (1981). The SNAP rating
scale. Resources in Education.
Sterman, M.B. (1980). EEG biofeedback in the treatment of epilepsy:
an overview circa 1980. In Leonard White and Bernard Tursky (Eds.),
Clinical Biofeedback: Efficacy and Mechanisms. New York: Guilford
Press.
Tansey, M.A. (1990). Righting the rhythms of reason. EEG biofeedback
training as a therapeutic modality in a clinical office setting.
Medical Psychotherapy, 3, 57-68.
Ullman, R.K., and Sleator, E.K., (1986). Responders, nonresponders,
and placebo responders among children with Attention Deficit Disorder.
Clinical Pediatrics, 25, 594-599. |